
Source: Unsplash/Louis Reed.
In particular, mass vaccination seems to have been relegated to a secondary issue; something we can see in the slow rate of supply, rollout and publicity.
Keeping people safe from COVID-19 through border restrictions has been very popular because it’s meant that most Australians are able to go about their normal lives (with the exception of international travel) without significant restrictions on their freedom and mobility within Australia.
But global elimination of COVID-19 is a very long way off, and border restrictions at their current levels are not sustainable.
In order to progress, it seems very clear that there needs to be parallel policies aimed at increasing vaccination rates much more quickly in Australia, stronger (and more) residential quarantine facilities including home quarantine for those vaccinated, coupled with gradual easing of border restrictions.
Carrots, sticks or nudges?
Even if there are enough vaccines available, persuading more people to get vaccinated can be difficult.
But there are many ways to help increase vaccination rates. Most seem to rely on social norms and peer pressure. If all of your friends or work colleagues are getting vaccinated and talking about it, then you are more likely to get vaccinated.
Fear of being ostracised from your group suggests that there are ‘social’ penalties if you do not get vaccinated. This can happen in workplaces, social settings, families, religious, ethnic, and political groups.
But a crucial issue in influencing social norms is information about the benefits and risks of vaccination, how individual vaccination also benefits others and how these information campaigns are targeted to these social settings.
Our previous research has shown that health professionals are the most trusted in delivering information, with celebrities and politicians the least trusted.
To implement strong interventions that influence social norms in every community in Australia is costly and will take time. There are many different population groups who are hesitant, so even a targeted policy will be difficult to implement nationally.
Given we are likely to be living with the risk of infection for some time, long-term investment that influences social norms is necessary — but does depend on its cost-effectiveness.
However, there are also short-term imperatives and a growing impatience about the time it is taking to get Australians vaccinated, coupled with persistently high rates of vaccine hesitancy (see Figure 1).
But there are other carrots, sticks and nudges that can be used — including not being able to travel if you are not vaccinated or not being able to go to work if employers require vaccination.
We know that losing something has more of an impact on behaviour than gaining something, and penalties like this could increase vaccination rates among those who are hesitant. Losing our freedom to travel, to go shopping, or go to restaurants is something we all experienced during lockdown and do not want to experience again.
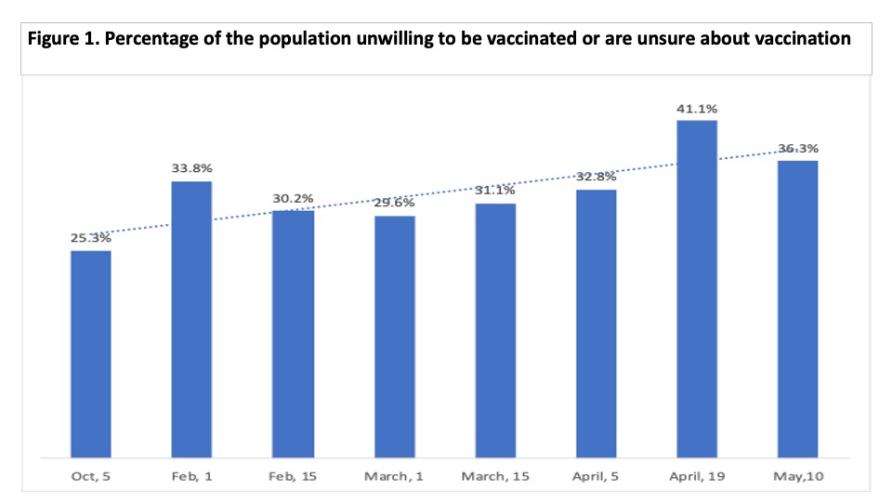
Source: Taking the Pulse of the Nation Survey/ Melbourne Institute: Applied Economic and Social Research. Based on 1200 nationally representative respondents per wave (Waves 20, 26-32). Taken from the question: Are you willing to be vaccinated: ‘yes’, ‘no’, ‘don’t know’. Excluded those from Wave 29 (March 15th) who answered yes to an additional option: ‘I have already been vaccinated’. Figures include those who answered ‘no’ and ‘don’t know’. Graphic: supplied
During lockdown, there was also the threat of fines if these rules were broken. Living with the risk of COVID-19 and its new variants will require a continuing degree of restriction — like QR codes, mask wearing, snap lockdowns and stronger quarantine.
So carrots, sticks and nudges have already been used to change behaviours, albeit under a state of emergency.
Why don’t we pay people to get vaccinated?
Right now, the incentives to get vaccinated are all wrong. Why should people bother to get vaccinated now if they can’t travel anyway until mid-2022 or later, or if their ‘preferred’ vaccine doesn’t get here until 2022?
There is little downside to waiting, but there could be more of an upside in getting vaccinated now.
Governments have been putting plenty of money into peoples’ pockets to stay employed and providing travel vouchers go on holiday. Why can’t we pay people to get vaccinated?
If you provide proof you have had your second jab, then people should be able to claim, say $50.
The website blueprint for a scheme like this exists through the Victorian Travel Voucher Scheme, or it could be implemented through Medicare and the Australian Immunisation Register or Centrelink.
Vaccinating 10 million people would cost $500 million at $50 to complete your first two jabs, or it could be targeted to certain sub-groups. The $500 million could be recouped quite quickly if it enables an earlier return to trade, tourism, immigration and international students.
Our previous reviews into using financial incentives in health care, especially for single ‘one-shot’ types of visits like immunisation, suggest they are effective.
Using financial incentives is not new and they work
We pay people through the tax system to take out private health insurance.
Governments are already using financial incentives to encourage childhood immunisation through families not being able to claim family tax benefit or not being able to send their children to childcare (‘no jab no pay’ and ‘no jab no play’).
In fact, governments even offer financial incentives if you change your electricity or gas provider.
There are many examples of successful cash transfer programs that encourage healthcare check-ups and school attendance in low and middle-income countries.
For many people who are hesitant or just waiting it out, financial incentives could nudge them in the right direction and get us where we want to be more quickly.
This article was first published on Pursuit. Read the original article.
ABOUT THE AUTHOR
Handpicked for you

Richard Branson says Australia’s slow vaccine rollout hurts all businesses — these startups agree



COMMENTS
SmartCompany is committed to hosting lively discussions. Help us keep the conversation useful, interesting and welcoming. We aim to publish comments quickly in the interest of promoting robust conversation, but we’re a small team and we deploy filters to protect against legal risk. Occasionally your comment may be held up while it is being reviewed, but we’re working as fast as we can to keep the conversation rolling.
The SmartCompany comment section is members-only content. Please subscribe to leave a comment.
The SmartCompany comment section is members-only content. Please login to leave a comment.